


When the Headache Is Not What It Seems
You have tried everything. The over-the-counter pain relievers. The dark room and the cold compress. The careful tracking of what you ate, how much you slept, and how stressed you were. And still, the headaches return – sometimes dull and persistent, sometimes sharp enough to sideline your entire day.
What if the problem is not in your head at all?
For a significant number of people living with recurrent headaches, the true origin lies not in the brain or its surrounding structures, but in the cervical spine – the seven vertebrae, joints, nerves, and muscles that make up the neck. This category of headache has a clinical name: cervicogenic headache. And it is one of the most consistently misidentified pain conditions in adults.

Estimates suggest that cervicogenic headache accounts for roughly 15 to 20 percent of all chronic headache cases – yet it is frequently mistaken for tension headache, migraine, or simply “stress.” As a result, many patients spend months or even years managing the wrong condition, with treatments that provide no lasting relief because they are not addressing what is actually driving the pain.
Understanding cervicogenic headache begins with understanding the relationship between the cervical spine and the head – a connection that is more direct and more consequential than most people realize.
How the Neck Causes Headaches
The cervical spine and the brain share a deeply interconnected network of nerves. The upper three cervical nerve roots – C1, C2, and C3 – converge with the trigeminal nerve, which is the primary sensory nerve of the face and head. This anatomical overlap, known as the trigeminocervical nucleus, is the reason that pain originating in the neck can be perceived as a headache.
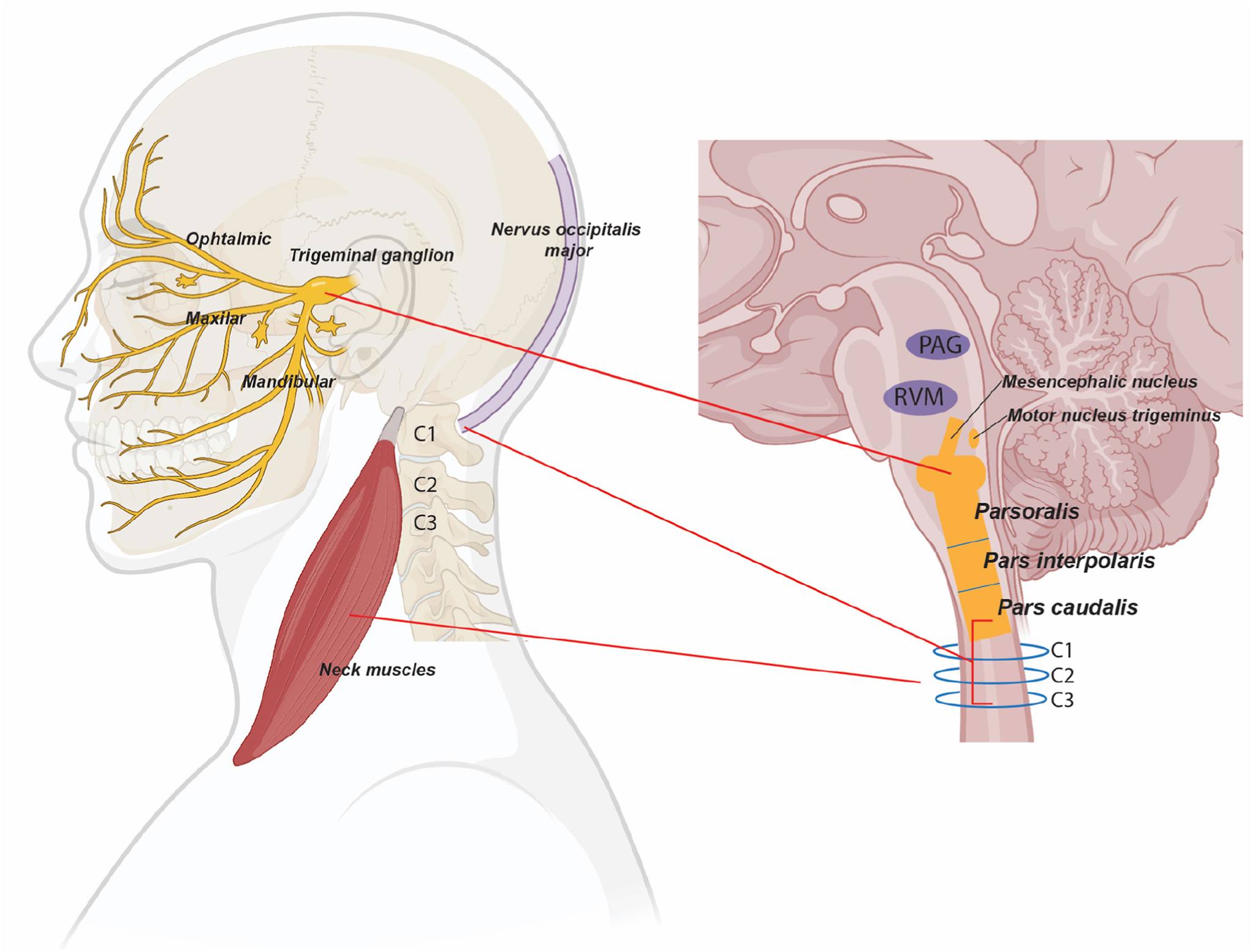
In practical terms: when structures in the upper cervical spine become irritated, inflamed, or compressed, the nervous system can interpret that pain signal as coming from the head – because the brain processes both sets of signals through the same pathway.
The cervical structures most commonly responsible for generating these headaches include:
- The upper cervical facet joints (C1–C3): These small joints at the top of the cervical spine are a frequent source of cervicogenic headache. Arthritis, inflammation, or joint dysfunction in this region can refer pain directly to the back of the head, the temples, and the area behind the eyes.
- The suboccipital muscles: The small muscles at the base of the skull – which connect the upper cervical vertebrae to the cranium – can become chronically tight and tender, particularly in people with forward head posture or prolonged desk work. Their sustained tension is a common driver of occipital headaches.
- Herniated or degenerated cervical discs (C2–C3): When disc material presses on nearby nerve roots in the upper cervical spine, the resulting nerve irritation can produce headache patterns that mimic migraine in their severity and distribution.
- The greater and lesser occipital nerves: These nerves travel from the upper cervical spine upward over the skull. When they become compressed or irritated – often by tight suboccipital muscles or by structural changes in the upper cervical spine – they can cause a distinctive radiating headache that travels from the base of the skull to the forehead.
What all of these sources have in common is that they are structural. They are not triggered by hormonal shifts, dietary factors, or light sensitivity in the way that migraine often is. They are driven by what is happening in the cervical spine – and that distinction matters enormously for treatment.
Cervicogenic Headache vs. Migraine vs. Tension Headache
Because cervicogenic headache shares symptoms with other common headache types, accurate identification is essential before any treatment plan is developed. Here is how these conditions typically differ:
- Location and pattern of pain:
Cervicogenic headache almost always begins at the base of the skull or the back of the head, then radiates forward – often to the forehead, the temple, or behind one eye. Migraines can begin anywhere and tend to be throbbing and severe. Tension headache typically produces a diffuse, band-like pressure across the forehead and temples.
- Relationship to neck movement:
This is the most clinically significant distinguishing feature of cervicogenic headache. If your headache consistently worsens or is provoked by specific neck positions – looking over your shoulder, tilting your head back, or remaining in one position for an extended period – the cervical spine is almost certainly involved. Migraines and tension headaches are not typically position-dependent in this way.
- Side of the head affected:
Cervicogenic headache is usually one-sided, and it tends to remain on the same side. Migraines can alternate sides. Tension headache is typically bilateral.
- Associated symptoms:
Migraines commonly produce nausea, vomiting, and extreme sensitivity to light and sound. Cervicogenic headache may cause some light sensitivity, but nausea and photophobia are generally less pronounced. Patients with cervicogenic headache more commonly report neck stiffness, reduced range of motion, and shoulder or arm discomfort accompanying the headache.
- Response to pain medication:
Standard headache medications – including triptans, commonly prescribed for migraine – often provide minimal or inconsistent relief for cervicogenic headache. If you have found that your headaches respond poorly to typical treatments, this is a meaningful clinical clue.
It is worth noting that cervicogenic headache can coexist with migraine in the same patient, which can complicate diagnosis. This is precisely why a thorough clinical evaluation – rather than self-diagnosis – is the appropriate path forward.
When to Seek a Professional Evaluation
Many people with cervicogenic headache have already navigated a long road by the time they reach a pain specialist. They have seen their primary care physician. They may have tried physical therapy, chiropractic care, or a neurologist. Some have been told their imaging is “normal” and that nothing structural appears to be causing their symptoms.
Normal imaging does not mean the cervical spine is not the source of your headaches. Many of the structural contributors to cervicogenic headache – particularly facet joint dysfunction and myofascial tension – are not reliably captured on standard MRI or X-ray. Diagnosis often requires a comprehensive clinical examination combined with diagnostic nerve blocks that can confirm or rule out specific cervical structures as the pain source.
The following signs suggest it is time to pursue a professional evaluation specifically focused on the cervical spine as a headache source:
- Headaches that begin at the base of the skull or the back of the neck and radiate forward
- Head pain that worsens with neck movement or sustained neck postures, such as looking at a screen
- A history of neck pain, whiplash injury, or cervical spine problems, alongside chronic headaches
- Headaches that have not responded adequately to migraine medications or standard headache treatments
- Restricted neck range of motion that correlates with headache onset or severity
- Headaches accompanied by shoulder tension, arm discomfort, or a heavy feeling in the head and neck
At Sun Pain Management, the evaluation of cervicogenic headache involves a detailed history, a targeted physical examination of the cervical spine, and – where appropriate – diagnostic procedures to identify which specific structures are contributing to your symptoms.
Treatment options may include:
- Cervical medial branch blocks: Injections that deliver anesthetic to the small nerves supplying the facet joints of the upper cervical spine. If a block provides significant temporary relief, it confirms the facet joint as a pain source and opens the door to longer-lasting treatment.
- Radiofrequency ablation of cervical medial branch nerves: When facet joints are confirmed as the headache source, radiofrequency ablation uses heat energy to interrupt the pain signals from the responsible nerves – providing relief that can last from several months to over a year.
- Greater and lesser occipital nerve blocks: Targeted injections around the occipital nerves at the base of the skull, used both diagnostically and therapeutically for patients with occipital headaches and cervicogenic patterns.
- Cervical epidural steroid injections: For headaches driven by upper cervical disc pathology or nerve root irritation, targeted anti-inflammatory treatment can significantly reduce both the frequency and severity of episodes.
Each treatment plan is individualized – because the cervical structures responsible for your headaches may be different from another patient’s, and because meaningful relief depends on treating the right source with the right approach.
If you have been living with headaches that have resisted conventional treatment, or if your headaches are accompanied by neck pain and stiffness, a cervical spine evaluation may be the clinical step that has been missing from your care.
You do not have to accept chronic headaches as simply part of your life. At Sun Pain Management, our team specializes in identifying the structural sources of pain that other approaches may have missed – and in building precise, personalized treatment plans designed around your specific anatomy and experience.


